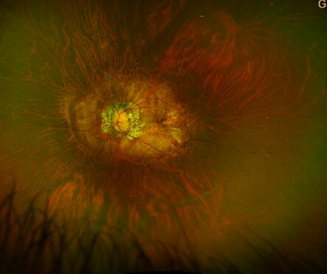
The development of these networks can vary, some may self resolve, or may cause bleeding.
In approximately 40% of cases, the new blood vessels regress, and the sea-fan resolves on its own. In other cases, the sea-fans do not exhibit significant growth and do not bleed.
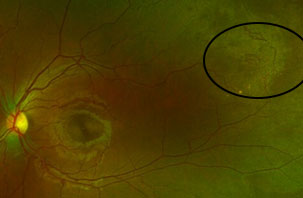
Proliferative sickle cell retinopathy is more common in individuals with HbSC type of sickle disease than HbSS. Majority have be asymptomatic in early stages, but some may unfortunately have temporary or more rarely, irreversible sight loss.
Sight loss from proliferative sickle cell retinopathy happens from vitreous haemorrhage which is a bleed from new bleed vessel into the vitreous gel or retina detachment where the retina seperates due to new blood vessel pulling on the retina (traction).
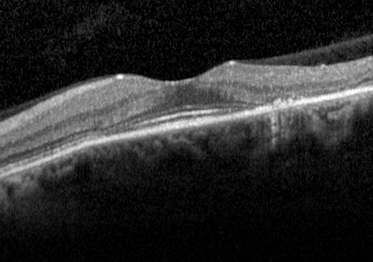
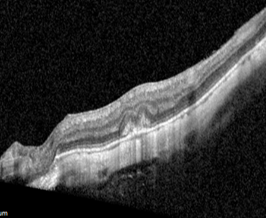
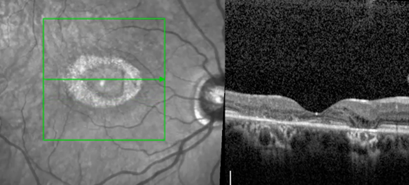
Other effects of sickle cell retinopathy include sickle cell maculopathy- where blood supply is lost in the macular or center of the retina causing demise of some of the photoreceptor cells and vision loss, retina artery occlusion where there is occlusion of the arteries delivering blood and oxygen to the retina.

 English
English